Articles
What is ptosis?
Droopy eyelids, also known as ptosis, can make the eyes look tired or uneven. Many people want to correct this condition without undergoing invasive surgery. Fortunately, several non-surgical and minimally invasive options can help lift and rejuvenate the eyes — from Botox and fillers to non-incisional ptosis correction.
Ptosis can lead to a tired and sleepy appearance, as well as blocked upper visual fields. As this gets worse, the forehead muscles can be activated to help compensate in a small way, but this can eventually lead to forehead creases and headaches. Simultaneously, the double eyelid crease can loosen and disappear. In severe cases, ptosis obstructs such a large part of the visual field that individuals start bumping into low-hanging objects or are unable to drive safely.
Causes of ptosis
The main cause of ptosis is involutional, or age-related, ptosis. This arises from the stretching of the muscles which lift the eyelid margin. There are two muscles that are responsible for this. The main muscle which lifts the upper eyelid is the Levator muscle, whilst the secondary muscle is the Mullers muscle. Both of these muscles attach to the cartilage plate present behind the skin and eyelashes, known as the tarsal plate.
Other causes of ptosis are congenital, mechanical (extra weight from a tumour or excess skin), myogenic (disease of the muscle itself), or neurogenic (when the nerves responsible for lifting the muscle are affected). In fact, a common cause of the latter two is Botox to the brow and forehead, whereby some of the Botox seeps to the upper eyelid muscle causing paralysis of the nerves and muscles which retract the lid. The upper eyelid should also be assessed in continuity with the brow, as a droopy eyebrow can lead to the appearance of ptosis due to the descent of skin between the brow and eyelid.
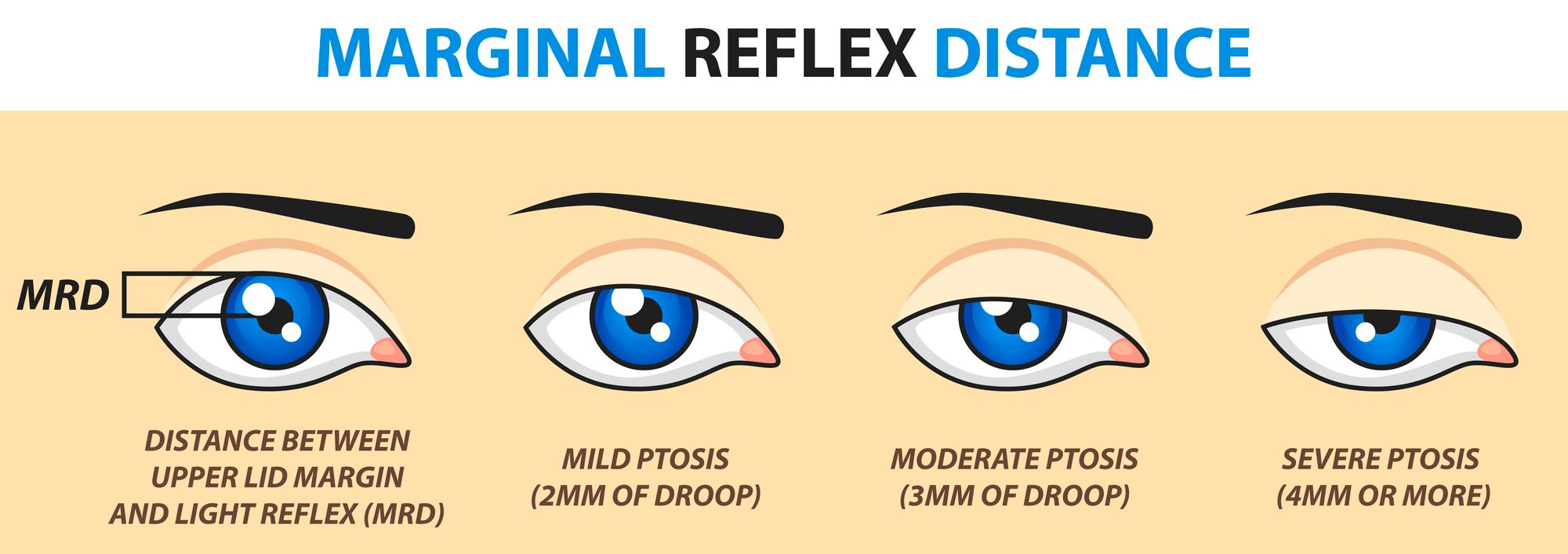
Ptosis can be a medical problem when there is significant blockage of the upper visual fields. This is measured by the MRD1, and by a formal visual field test. Your plastic surgeon will be able to advise you regarding this.
How is ptosis treated?
Mild forms of ptosis or ptosis secondary to brow droop might be resulted in ptosis correction without surgery by Botox to the muscles responsible for lowering the brow or closing the eye. However, these effects are often mild and are not permanent.
The management of ptosis largely relies on procedures to reverse the cause of the ptosis. In most cases, this involves the tightening of the muscle responsible for lifting the upper eyelid margin. This can be done via an incisional approach to visualize the Levator muscle and directly tighten it, or via a non-incisional approach where sutures are placed through the skin and Mullers muscle using precise measurements to avoid having to make a cut, which leads to no scar. The incisional approach, whilst allowing for full control over the upper eyelid structures, can lead to visible scars and is associated with longer bruising and swelling. In severe cases of ptosis where there is no Levator or Mullers muscle function, the muscles of the forehead may have to be recruited to help with lifting the eyelid margin.
As a bonus to correcting ptosis, these procedures also help with creating an attractive double eyelid.
Ptosis correction without open surgery
Ptosis correction can be performed via a non-incisional approach by utilizing needles and fine sutures placed through the skin and cartilage of the upper eyelid, simultaneously shortening the Mullers muscle which is used to raise the upper eyelid margin. By shortening this muscle, it automatically lifts the eyelid margin. Placing these sutures also creates a double eyelid crease, and similar methods are used in non-incisional double eyelid procedures.
This form of ptosis correction leaves no scars, can be performed under local anaesthesia, and is quick to perform in clinic, often taking much less than an hour for both upper eyelids. It is associated with less bruising and swelling than the incisional method of ptosis correction. However, the extent of ptosis correction is not as much as Levator muscle surgery, and the risk of recurrence is higher, therefore it is usually reserved for cases of milder or moderate ptosis, and for cases where skin or fat does not need to be removed.

Non-Surgical Treatments for Droopy Eyelids
Before considering surgical or non-incisional correction, mild cases of droopy eyelids can often be improved through non-surgical treatments. These methods are ideal for those seeking subtle or temporary lifting effects.
Botox for Droopy Eyelids
Botox relaxes the overactive muscles around the eyes that pull the eyelids downward. This can create a gentle lift, especially around the outer corners of the eyes.
Dermal Fillers for Eyelid Lift
Hyaluronic acid fillers can restore lost volume around the upper eyelid and brow, creating a smoother, lifted appearance without surgery.
Eyelid Creams and Serums
Peptide- and caffeine-based eye creams can temporarily tighten and brighten the skin around the eyes, offering a mild lifting effect.
What should I expect from non-incisional ptosis correction?
Non-incisional ptosis correction is an office-based procedure that can be performed in under an hour. The procedure is done under numbing eyedrops and local anesthesia injection to the skin, and besides the pinprick at the moment of injection, is remarkably comfortable. During the procedure, your eyes will be closed. The needles and sutures used for the procedure are very small and will not be felt after the surgery. Bruising and swelling are minimal, which dramatically shortens downtime, and by 2 weeks after surgery almost all the swelling would have resolved. There are no sutures to be removed, and you will be given antibiotics to reduce the risk of infection after the procedure, as well as painkillers to control any pain which may occur after the local anaesthesia wears off. Again, these risks are very minimal.
When Surgery May Be the Best Option
While non-surgical and non-incisional options work well for mild to moderate cases, surgical ptosis correction may be necessary for severe or functional eyelid drooping. A consultation with a qualified plastic surgeon helps determine which approach is best for your needs.
Considering a droopy eyelid correction?
Book a consultation with Polaris Plastic Surgery to explore your options — from non-surgical lifts to non-incisional and surgical correction methods tailored to your needs.
At Polaris Plastic & Reconstructive Surgery, we provide the highest standards of plastic, reconstructive and aesthetic surgery services to suit the individual needs of each of our patients, placing their well-being and concerns at the center of a seamless, holistic interaction with our practice.
Visit us at
1 Orchard Boulevard #10-08 Camden Medical Centre, Singapore 248649
1 Orchard Boulevard #10-08 Camden Medical Centre, Singapore 248649
3 Mount Elizabeth, #08-09 Mount Elizabeth Medical Centre, Singapore 228510
6 Napier Rd, #08-01 Gleneagles Medical Center, Singapore 258499
Tel: +65 6737 4565 | Mobile: +65 8828 4565 | Email: clinic@polarisplasticsurgery.com | Business Hours: Mon - Fri: 9am - 6pm | Sat: 9am - 1pm | Sun/Ph: Closed
6 Napier Rd, #08-01 Gleneagles Medical Center, Singapore 258499
Tel: +65 6737 4565 | Mobile: +65 8828 4565 | Email: clinic@polarisplasticsurgery.com | Business Hours: Mon - Fri: 9am - 6pm | Sat: 9am - 1pm | Sun/Ph: Closed
Insurance Panels