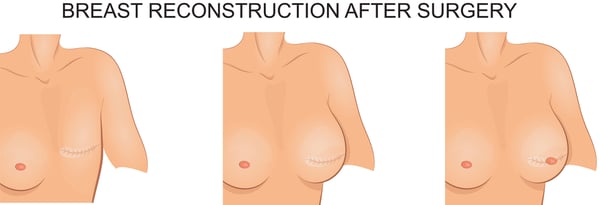
How is breast reconstruction performed?
Breast reconstruction can either be performed with implants, or with your own tissue (autologous reconstruction). There are many pros and cons to both. Generally, implants (including expanders) provide a faster form of reconstruction with no additional donor sites but can be more prone to infection and later problems such as capsular contracture. In addition, despite advances in implant technology, they do not feel as natural as your own tissue.
Traditionally, breast implants have been placed behind the pectoralis major muscle for breast reconstruction. But in recent years and with development in materials such as acellular dermal matrix, placing the implant under the skin and in front of the muscle, (pre-pectoral breast implant reconstruction), which is the natural plane of breast tissue, has gained increasing popularity, and our surgeons are very familiar with these procedures.
Autologous reconstruction borrows tissue from another part of your body to reconstruct the breast and can be performed with the blood supply attached (pedicled reconstruction) or by reattaching the blood supply at the breast (free tissue transfer). Tissue can be taken from many areas where there is excess skin and fat, most commonly the abdomen, but also from the back, thighs, and buttocks. The most common forms of autologous reconstruction are the Deep Inferior Epigastric Perforator (DIEP) and Transverse Rectus Abdominis Myocutaneous (TRAM) flaps, which can either be performed as a pedicled or free flap. Autologous reconstruction provides the most natural and lasting method of reconstruction, but often takes longer and results in donor site scars. These scars, however, can be well hidden.
After the initial reconstruction, your surgeon may recommend additional procedures such as nipple reconstruction and other touch-ups to enhance symmetry and appearance. Secondary problems resulting from breast cancer treatment, such as lymphedema and radiation injury, can also be treated at the same time as the reconstructive surgery, or later.
At Polaris Plastic and Reconstructive Surgery, our board-certified plastic surgeon will be happy to perform a thorough assessment and discuss the appropriate options for your breast reconstructive surgery. Dr Adrian is sub-specialist trained in all forms of breast reconstruction and fellowship certified specifically in free DIEP and TRAM flap procedures, areas in which he is well published.
At Polaris Plastic & Reconstructive Surgery, we provide the highest standards of plastic, reconstructive and aesthetic surgery services to suit the individual needs of each of our patients, placing their well-being and concerns at the center of a seamless, holistic interaction with our practice.
Visit us at
1 Orchard Boulevard #10-08 Camden Medical Centre, Singapore 248649
1 Orchard Boulevard #10-08 Camden Medical Centre, Singapore 248649
3 Mount Elizabeth, #08-09 Mount Elizabeth Medical Centre, Singapore 228510
6 Napier Rd, #08-01 Gleneagles Medical Center, Singapore 258499
820 Thomson Rd, #06-68 Mount Alvernia Medical Centre, Singapore 574623
Tel: +65 6737 4565 | Mobile: +65 8828 4565 | Email: clinic@polarisplasticsurgery.com | Business Hours: Mon - Fri: 9am - 6pm | Sat: 9am - 1pm | Sun/Ph: Closed
6 Napier Rd, #08-01 Gleneagles Medical Center, Singapore 258499
820 Thomson Rd, #06-68 Mount Alvernia Medical Centre, Singapore 574623
Tel: +65 6737 4565 | Mobile: +65 8828 4565 | Email: clinic@polarisplasticsurgery.com | Business Hours: Mon - Fri: 9am - 6pm | Sat: 9am - 1pm | Sun/Ph: Closed
Insurance Panels